Definition
‘Soft’ Interoperability or copy-and-paste friendliness is a form of technology workaround employed by users when true technical interoperability is not available. It is usually encountered when transferring small amounts of data between different clinical records systems, or between a clinical record system and an external clinical tool.
Origin
I coined this term in approxiimately 2020 when working on the RCPCH Digital Growth Charts - when we were building the graphing user interface we considered that while we encouraged a full technical API level integration, not every implementation would achieve that. We didn’t want to make life harder for the clinicians who worked in those latter, less digitally mature, settings.
Advantages
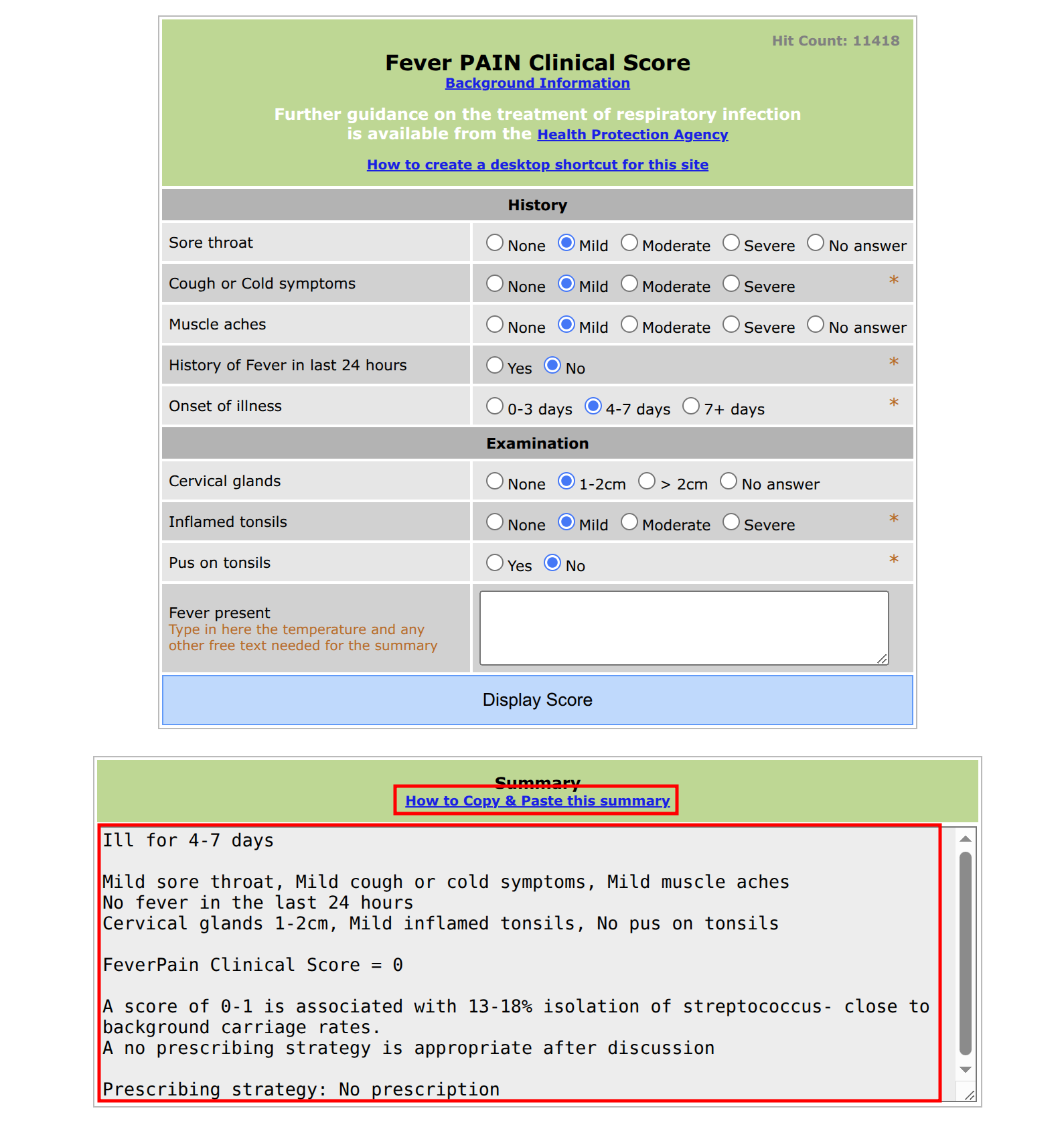
In the design of clinical systems and ancillary services such as clinical calculators, soft interoperability can be facilitated in the design of the system. In the FeverPAIN example below, it is facilitated by generating a helpful synopsis of both the input data and output advice, and making this easy to copy to the clipboard.
While soft interoperability is less desirable than true technical interoperability through standardised interfaces such as APIs, it can still reduce ‘clinical drag’ (the loss of productivity caused by systems that do not facilitate the clinical process). The alternative is the user having to manually transcribe the data from one system to another. Copy and paste of data is definitely less prone to typographical error than manual entry. It can also provide at least a simple level of standardisation of the data that is entered, which is surely better than leaving this to individual clinicians.
However, there is often hesitation within the digital health and clinical informatics professions to enable soft interoperability in systems, or even acknowledge that it is a valid mode of operation - because it represents a tacit admission that ‘true interoperability’ has failed to be instituted between the systems.
As a clinician though, I think it is preferable to have soft interoperability than no interoperability. When we implement clinical systems, it is important to consider that implementations are not always perfect, and we shouldn’t let perfection stand in the way of acceptable but less perfect workarounds.
Disadvantages
The availability of a soft interoperability workaround like this could conceivably be used as a reason not to implement a more digitally mature, technically implemented end-to-end interoperability solution.
Example - FeverPAIN online clinical calculator
During my GP training I recall encountering the FeverPAIN clinical calculator website, and noticed that it has been built to make it easy to copy and paste the outcome into another system.
The team who produced this website clearly knew that there was never realistically going to be a ‘true interoperability’ integration between this site and any electronic medical record, so they made it easy to transfer the result into the medical record. Copy and paste works everywhere.
Fever PAIN Clinical Score FeverPain
References
I wasn’t sure if I was the first person to coin the term “Soft Interoperability”, so I did a bit of research:
Soft interoperability is mentioned here in this paper about sharing GIS data across organisational boundaries. https://www.sciencedirect.com/science/article/abs/pii/S0303243401850352
Here it is used differently, in a podcast by Nordic - they are using it to mean ‘everyone agreeing to use the same EHR’ which is of course just monopoly. DocTalk Ep. 105 | Soft interoperability | Nordic Global