Medical handover takes various forms depending on speciality and location, acuteness of patients/illness severity, etc. It follows a similar pattern to the army watch handover though - what you’ve done, what needs to be done. I’ll try to bash out a few bullet points here, and I’m hoping to be able to obtain some real paper handover sheets to help illustrate.
-
Usually handover would be 12-hourly as one shift hand over to the next shift. In some areas where the shifts are shorter (eg ED) then handover would be 8-hourly. Handover can last anything from just a few minutes (eg ED when it’s inexplicably super quiet) to a full hour (eg on an ICU), depending on the amount that needs to be handed over.
-
When I started medicine this would be a handwritten list, each doctor would make and maintain their own copy. If you were on all weekend for example, you could just update yesterday’s list in some places since the patients may well be the same.
-
Later on (say 2005 onward) the default started to be a Word document (a table) or an Excel spreadsheet, where each row would be a patient, and the columns would be their details. Each team member would generally still print out a hard copy, which they would annotate and add to as they worked clinically (much of our work is away from the computer) then they would update the Word version
-
For most hospital specialities we would go through a list of the patients that service is caring for. This ‘patient list’ feature is the thing that a lot of EPRs just don’t support well. We need to be able to add and remove from this list easily.
-
It’s also important that we can easily make notes and changes across the whole of the list without having to go into each patient’s actual EPR as this is time consuming.
-
In some places the handover documents are an organisational safety/clinical governance record that a handover meeting took place and the sheets may actually be signed, dated, and kept. In other places the handover sheets are shredded once the shift is over. (And of course a small proportion accidentally taken home, left on buses, found in the bottom of work bags after moving on to the next rotation, turned to mulch in the washing machine…)
-
The ‘digital master’ can be a blank document which is simply printed and populated with handwriting. However, in some care settings it can be a digital document which is kept updated with actual patient information and a new version of the file is saved to the PC. This practice is discouraged because of the IG risks posed.
Advantages of paper documents
(ie a paper handover sheet, with or without some form of digital ‘master’ that is updated later)
- Easy to update using a pen or in bulk on the computer
- Portable, light, easily carried in scrubs
- Multi-user
- Requires no proximity to a computer
- Body fluid resistant
- If damaged or lost, cheap to replace - print another.
- Easily managed and edited by anyone with simple Word-level computer skills.
Disadvantages of paper documents
(ie a paper handover sheet, with or without some form of digital ‘master’ that is updated later)
- HUGE information governance concerns - a single handover sheet if lost would disclose confidential information about many patients.
- Double or triple entry of data - all the handwritten updates need to be copied back to the digital master and the patient’s EPR.
- Data might change during the day, and other team members will have outdated information on their copy of the handover sheet.
DON’T BREAK USERLAND As you can tell from all of the above, it is a real mess at the moment, from many perspectives. But whatever solution replaces these ad-hoc arrangements MUST NOT BREAK CLINICAL WORKFLOWS. Because, bad as these handover forms may be, they are working, and we clinicians will have to continue to deliver clinical care with whatever replaces them. ‘Don’t Break Userland’ quote source
Writing all this I’m actually just quite amazed that despite all the money that’s been poured into NHS tech in the past 20 years, the current state of handovers - a fundamental part of safe medicine - is so poorly handled as to show no evidence that anyone has ever tried to solve it.
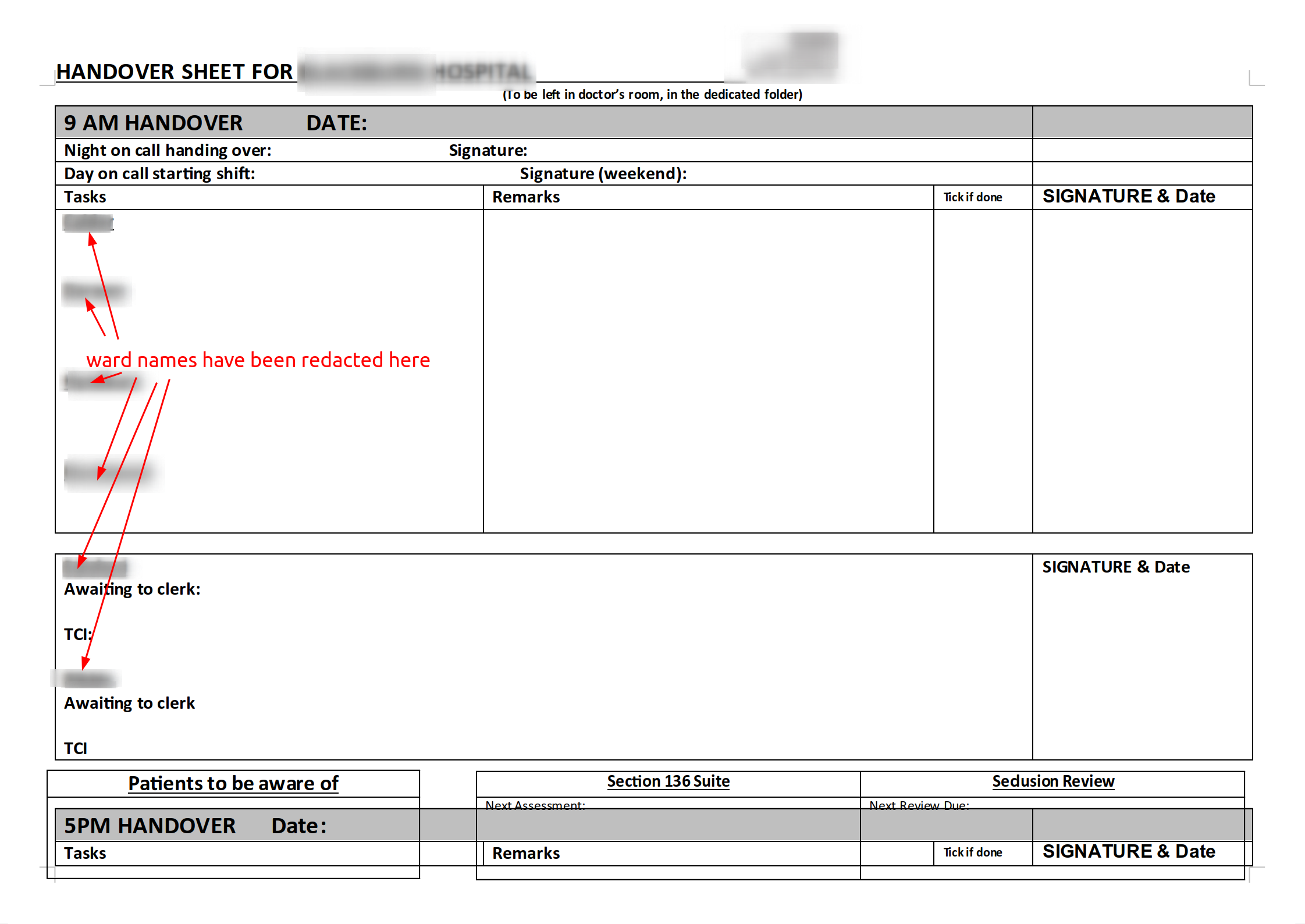
Images of some handover documents
Psychiatry
Critical Care (ICU)

Resources / Links
- JP Lomas has published the templates from some handover sheets here GitHub - jplomas/handover.xls: My (in)famous ICU handover spreadsheets
If anyone’s interested, I could go on to try to delineate some of the general principles that might form part of a digital solution to handovers…