I’m looking for some help!
Personal background: I’m a consultant neonatologist at the Evelina in London and an MIO.
Context: Neonatal units have for many years (decades) used a system called BadgerNet as a hybrid national neonatal EHR and national reporting platform - all units at some point used BadgerNet as an EHR-lite which allowed visibility of patient information throughout the patient journey (moving from unit to unit) and the same data for national benchmarking and research could be picked straight out of the BadgerNet back-end.
Problem: Forward to 2025 - the vast majority of neonatal units have now come off paper and are using a full EHR system, in some cases this is the full BadgerNet suite which allows direct data capture - in other cases it’s a.n.other EHR. Now we have the problem of how we ensure data from these systems still gets to where it needs to. The BadgerNet team have offered a data schema for external systems to send data into the BadgerNet system - it’s an XML wrapper with some data structure but is not FHIR based and is not the complete dataset, it’s also often not complete.
Having pushed this issue with colleagues in NHEE and SystemC (the owners of BadgerNet) SystemC have agreed to create FHIR profiles that other vendors can use.
The advice I’m looking for is how do we ensure that this is a sustainable and workable solution - owned by the community? Should we ask NHS England to own the databse for neonatal data rather than BadgerNet/SystemC? Thoughts?
Sounds like an really interesting problem.
How many systems are involved? What suppliers are they.
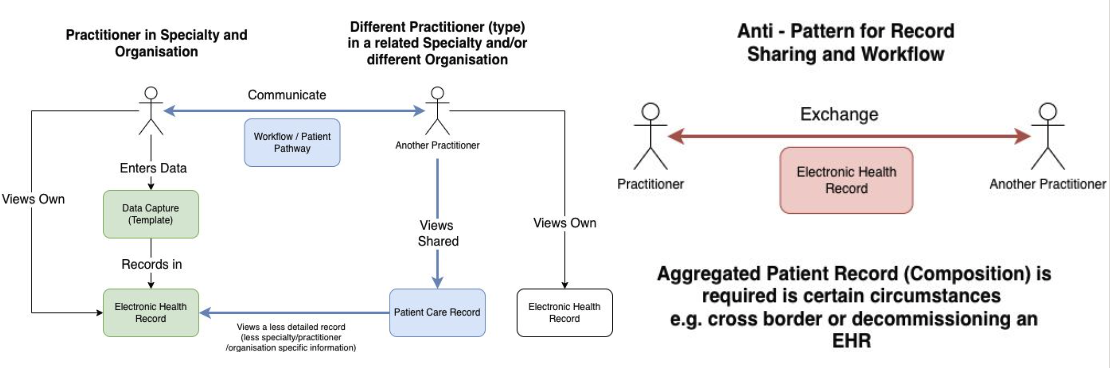
The method badgernet is possibly old fashioned (tech version = anti pattern), the modern method would be for all systems to share the data (for all practitioners) in a consistent way (is no send unless it is workflow related).
Who uses the master database? Is this for research and analytics
Is PRSB Digital Maternity describing the data at a high level PRSB Standards
This probably needs to be broken down into data capture templates (screens or forms) - you probably know what these are.
The next step after this is probably where I’d know most. Step before might be @ian @shanemuk etc
Note: I would suggest or highly recommend not thinking what the computer systems are until we’ve got an idea on the data models and processes/workflow involved. I think this can be engineered correctly and avoid all the mistakes we normally make.
Thanks Kev,
Lots of systems, EPIC, CERNER, SystemC and some smaller vendors.
I agree that an approach that involves sharing from all makes sense - it has to sit somewhere and at teh moment that somewhere is by defaults SystemC/BadgerNet. The database is used by the Royal college of Paediatrics for benchmarking/audit, NHSEngland for activity and by a research team for research (Neonatal research database).
PRSB doesn’t describe this dataset (there’s a smaller dataset of neonatal data embedded within maternity data that is PRSB described but it doesn’t include care on a neonatal unit).
Front end data capture form are obviously going to be vendor specific (albeit with an agreed standard for data format) - we’ve done this for Epic in our site (PITA).
I agree that this needs to be vendor agnostic and driven by the clinical/data needs but I need to bring everyone to the table and get them to play ball!
Hi @drhammadkhan and thanks for posting an important question.
It does make sense to have standardised data structures for putting data into (and getting it out of) BadgerNet. If they have something XML based then that is a start, although as you say it would make more sense to use FHIR for this, which is now well established as the de-facto standard for this kind of system-to-system interoperability.
RCPCH Incubator
I am one of the team at RCPCH’s ‘Incubator’ - we would be very keen to help out with ensuring the data standards were up to scratch. We have had conversations with other BadgerNet and SystemC sites regarding Digital Growth Charts and we would be able to provide you some technical and organisational support. It sounds like you would be an ideal person to join our private RCPCH Incubator forum where we can discuss this. It’s (for the moment) invite-only, go here and I will approve your account. https://forum.rcpch.tech/
RCPCH might be a body which could help develop and share the data standards with SystemC/BadgerNet.
NHS England
I would not let NHS England do anything with anyone’s data at the moment. Reasons:
-
NHSE chaos. They are in complete internal disarray due to the announced abolition of NHSE which will take place over the next few years. Functions of NHSE will be absorbed into DHSC, but during these regular re-disorganisations often cause projects to be ‘orphaned’ - for example if the Senior Responsible Officer for a project/programme is moved, leaves, or is overwhelmed with other work, then entire projects can lose momentum or even be cancelled entirely. In short, a total mess.
-
Palantir FDP. Any data you ask NHSE to ‘look after’ is likely to end up in the Palantir-Foundry NHSE Federated Data Platform, which aside from its major ethical issues, is not necessarily designed for data for Direct Care purposes. It is meant to be a Planning and Analytics platform, but because these are Secondary Uses for the data (and have a requirement to honoour the Type1 Opt Out and National Data Opt Out, which they’d prefer not to) they have started to let the scope creep towards Direct Care (which has no requirement for Opt Outs). In short, a total mess.
-
SPR. The 10-Year Plan announced the plan for creation of a Single Patient Record (SPR) which aside from its announcement has not yet been publicly developed further as an idea. We know nothing about the planned architecture, scope, or timescale. We do know that the SPR announcement is the result of intense and persistent lobbying by the Tony Blair Institute, which receives a lot of funding from Oracle/Larry Ellison. So we are expecting that the technical provision will be Oracle-based.
PRSB
In theory PRSB is the ‘right’ organisation to develop and hold any standards for data interchange between systems. However they have just had their funding from NHSE cut off abruptly, which threatens the PRSB’s existence. Statement: The ending of the Core Information Standards Service (CISS) with NHS England - PRSB. I wouldadvise against investing significant time into working with PRSB in the current climate.
In part that’s good news. The data from EPIC and Cerner has probably been shared already using modern international standards. ← This is more technical but it puts the work on whoever is holding the database (i.e. the consumer), not the providers. If we ask EPIC or Cerner to do the work (producers), they will want paying or just give a flat no and technically, it can get quite horrid (for developers).
The standard PRSB have done might be good enough to work towards data interchange standards.
Is this your main use case?
It is already possible to start “hacking” this (as long as you don’t require to have a database as the solution).
A proof of concept would need access to EHR suppliers data sharing endpoints plus some application developers, they could start putting together a clinical portal/health information exchange tailored to your needs - probably within 1-2 days.
Thanks Marcus, I would love for this to be the approach with ownership by RCPCH - at them moment we are a little adrift. I know that Cheryl Battersby has given it some attention but no plans as yet. I will join the college forum. I would want ownership of the database to sit with the college ideally with a standards based approach to the data and for anyone to be able to access (with the right permissions/safegurds) so less gatekeeping.
Maybe some power from the government to support this.
Maybe.
May main worry is the choice of architecture, it is often decided quite early on.
NHS England tends to go for the red box (exchange) and NHS Trusts the blue boxes (workflow and data sharing APIs). The difference is technical but it’s worth bearing in mind COVID 19 Vaccination took the “blue pill” route, it scales.
Makes so much sense - thanks Kev
I used to work for NHS England and one the problems we had was that we weren’t given the user requirement and how the maternity worked (how practitioners interacted). We were often given data requirements (e.g. PRSB Maternity Information Standard - PRSB or a spreadsheet) and/or a description how computer systems fitted together.
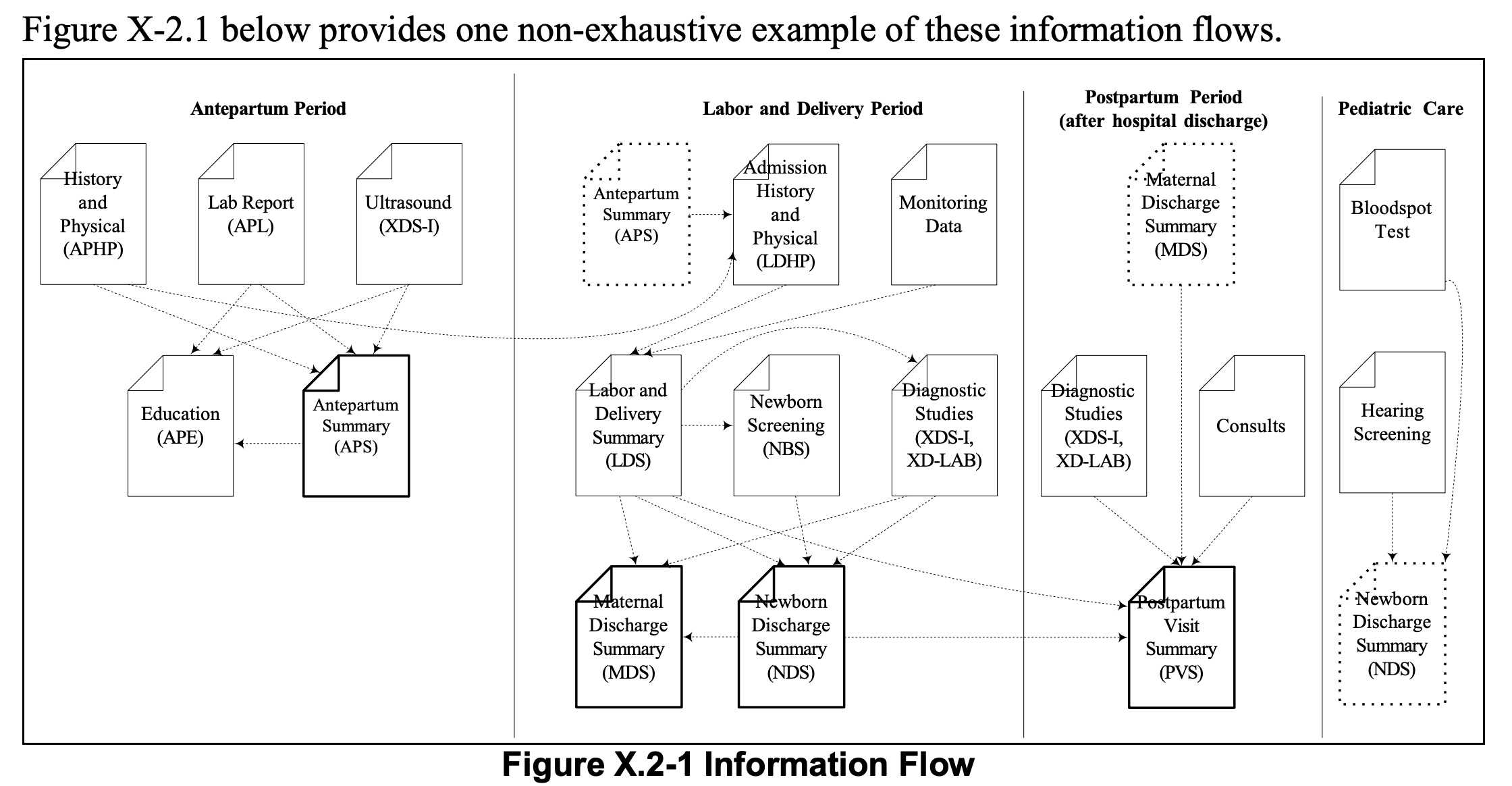
Personally I’d prefer to understand the processes (workflow) and high level data model. For example something like this
This may overlap with the PRSB but the data+process is broken down and is becoming more modular. This diagram is more geared towards getting maternity automated across multiple providers (i.e. patient journey and practitioners (and computer systems in particular), i.e. an enterprise.
It is not aimed at populating a central database (or EHR) but breakdown of data items would probably help with that. it does suggest solving maternity using a Health Information Exchange (HIE)/Clinical Portal instead.
It is a bit verbose in places , technical and several parts can be modernised (often using IHE+FHIR) but this does contain a number of user stories and other information a developer would find useful to understand the problem.